
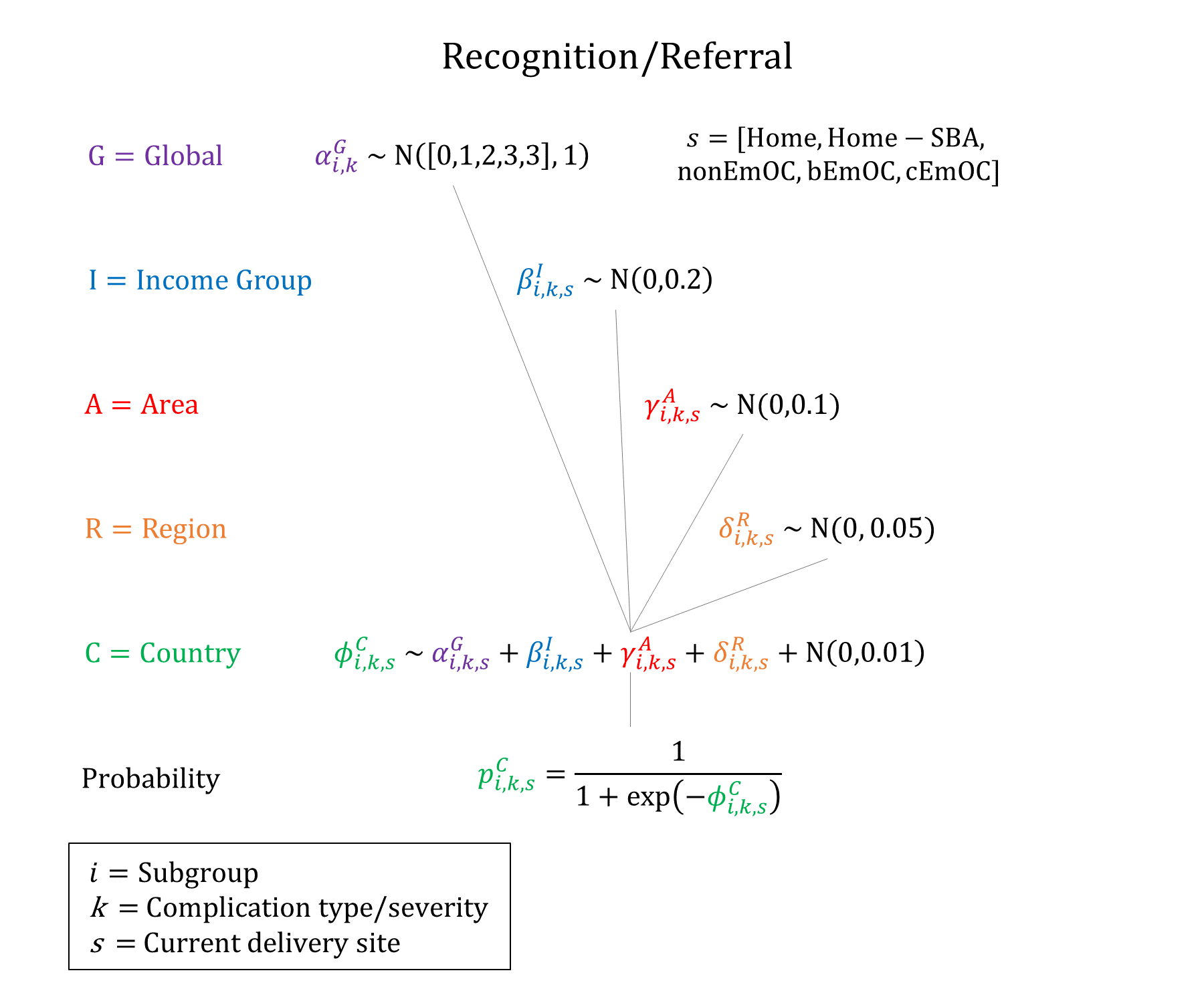
Recognition/Referral
Model Inputs \(\rightarrow\) Health System Parameters \(\rightarrow\) Recognition/Referral
Overview
In order to be treated, a complication must first be recognized, and perhaps referred to an appropriate facility. Recognition/referral of a complication is conceptualized as the “first delay” in the framework developed by Thaddeus and Maine.[1] We model different probabilities of recognition/referral by starting delivery site and complication type/severity.
The broader concept of recognition/referral encapsulates different aspects of complication management and health-seeking behavior such as: technical knowledge of complication danger signs, cultural acceptability of referral (ex: whether the husband is present and gives permission for the wife to go), financial barriers, childcare arrangements, etc. A systematic review found five main sub-themes related to the first delay: socio-economic factors, community perceptions about obstetric complications, women’s autonomy and insufficient male partner involvement in the management of obstetric emergency, maternal obstetric history and health service utilization, and women’s knowledge about obstetric danger signs.[2] These factors contributed to delays at home to seeking appropriate obstetric care in a timely manner when needed.
Data
We undertook a targeted literature review of recognition/referral pathways and women’s knowledge of obstetric danger signs, summarized by country below.
Bangladesh:
A study describing the process of recognition and response to symptoms during potential prolonged labour found that the most frequent and usually first action was to seek care from untrained attendants at home, followed from professional attendants outside the home, with care-seeking outside the home occurring a median of 19 hours after perceived labor onset.[3] Another study in rural Bangladesh of women who reported a ‘serious or very serious’ complication during their last pregnancy/delivery found that most women sought care for ‘serious’ complications (86%), with 42% seeking multiple sources of care.[4] A community-based cross-sectional survey in Matlab of women who delivered in 2014 found that 26% of women could recognize three or more pregnancy danger signs, and 23% could recognize three or more delivery danger signs.[5]
Ethiopia:
A systematic review and meta-analysis found that 32% (95% CI: 25.6-38.5) of pregnant women were prepared for birth and its complications, and only 26.33% of pregnant women were aware of danger signs during pregnancy.[6] Another systematic review and meta-analysis found that the level of women’s knowledge about obstetric danger signs during pregnancy, delivery, and postpartum was 48%, 43%, and 32%, respectively. Maternal age, education, income, health service use, distance from facility, and women’s autonomy were reported in several studies as determinants of women’s knowledge of obstetric danger signs.[7]
Ghana:
A household survey in East Mamprusi District found that 51.1%, 29.4%, and 34.6% of women knew at least three key danger signs during pregnancy, delivery, and postpartum period, respectively.[8]
Haiti, Malawi, Senegal:
A study of ANC clients based on service provision and assessment (SPA) surveys in Haiti, Malawi, and Senegal found that in all three countries more than half of clients knew at least one danger sign, but most clients could report only one, while almost no clients knew all seven.[9]
India:
A study of pregnant women attending the outpatient department of an urban tertiary care hospital for the first time found that 20%, 15.8%, and 12% had knowledge of at least 3 danger signs of pregnancy, labor, and severe illness in newborns, respectively.[10] A cross-sectional study of antenatal and postnatal mothers registered in a Rural Health Training Center in Kancheepruam district, Tamil Nadu found that 21% of women had adequate knowledge (correctly answering at least 6/12 questions) regarding the danger signs of pregnancy, with maternal literacy and adequate prenatal care major determinants of respondent knowledge.[11] Another study in Dakshina Kannada district, Karnataka found that 53.8% of women were aware of at least 6 danger signs.[12] A study in a rural block of Haryana found that >8 danger signs were known to only 9.5% of participants.[13] Studies have found that knowledge of danger signs is likely somewhat higher among trained birth attendants. A study of Accredited Social Health Activists (ASHAs) in a rural district in Karnataka found that 1%, 4.8%, and 7.2% were aware of all key danger signs for labor and child birth, postpartum period, and pregnancy period, with a majority (71%) scoring 4-7 out of 8.[14] A study in three states (Maharashtra, Rajasthan, and Odisha) exploring the adequacy of knowledge and clinical skills of ayurvedic and homeopathic practitioners engaged by the state governments to provide maternity care services found that nearly 76% had adequate theoretical knowledge of essential obstetric care and identification and management of complications of pregnancy.[15] Looking at actual responses to complications (not just general knowledge of danger signs), studies have found higher proportions of women who seek care. Using a broader definition of “complication”, the Coverage Evaluation Survey (CES) 2009-10 found that 32.8% of women who experienced a complication did not consult anybody, implying that the remaining ~70% of women did seek some form of care.[16] Similar findings were observed by Montgomery (2014): a study based on a nationally representative survey found that two-thirds of women died seeking some form of healthcare, with most seeking care in a critical medical condition - it also found that rural areas of poorer states had proportionately lower access to and utilization of healthcare services than in urban areas, but that this rural-urban disparity was not seen in richer states.[[17][Montogmery]] Another study found that out of 153 maternal deaths identified through community workers, verbal autopsies indicated that 23% occurred at home and that 30% occurred on the way to a health facility.[18]
Indonesia:
A study in Jayawijaya district, Papua province in eastern Indonesia, found that the decision to seek care lies predominantly with the husband. There was no significant lag time between the decision-making stage and the process of seeking care for the maternal cases. On average, the interval between symptom recognition and the decision to seek care in the home was less than 6 hours. Rapid decision-making usually occurred when visible symptoms of excessive bleeding began to appear.[19]
Kenya:
A study of women attending antenatal care at Kenyatta National hospital found that 67% of respondents knew at least one danger sign in pregnancy, while only 6.9% knew of three or more danger signs, with level of education positively influencing birth preparedness.[20] A CEmOC facility-based qualitative study of 30 women who experience obstetric “near miss” in Malindi found that 16/30 women experienced delays in making the decision to seek care, compared to 8 women who experienced delays in reaching the care facility, and 6 experienced delays in receiving care at the facility.[21] A community-based cross-sectional survey of community health workers/volunteers in North and East Kamagambo, Migori County found that 60% of participants in North Kamagambo knew 3 or more danger signs in 3 or more categories, compared to 24% of participants in East Kamagambo, revealing varying levels of knowledge among the two populations of lay health workers.[22]
Madagascar:
A convenience sample of 372 women in their first year postpartum between April-October 2015 found that knowledge of at least one danger sign varied from 80.9% of women knowing danger signs in pregnancy, to 51.9% at delivery and 50.8% postpartum, with women with higher education more likely to know danger signs.[23]
Malawi:
A study of primigravidae women in a rural health center in Blantyre found that 82% (95% CI 67-96) of women had some knowledge and could make an informed decision to go to a health facility with pregnancy complications, with 61% (95% CI 42-79) able to do so with complications after delivery.[24] A following study of primigravidae women in an urban health center found that 60% of the participants were knowledgeable about obstetric complications in pregnancy, however, 73% and 82.2% did not know of any problems that could occur during and after delivery, respectively.[25] Participants had limited knowledge of complications that may need immediate treatment during all three periods: 58% (95% CI 43-73) had some knowledge and could make an informed decision to go to a health facility with pregnancy complications, however only 24% (95% CI 11-38) could do the same for complications after delivery.[25]
Morocco & Netherlands:
A qualitative study to describe knowledge of hypertensive disorders in pregnancy among pregnant Moroccan women in Morocco and the Netherlands found that half of them had never heard about hypertension in pregnancy and had no knowledge of symptoms or alarm signals.[26]
Myanmar:
A cross-sectional survey of 262 auxiliary midwives from July 2015 to July 2016 found that only 8% were able to identify at least 80% of 20 critical danger signs, and 57.6% knew three or more critical danger signs during pregnancy, and 54.2% knew four or more critical signs during birth and postpartum.[27]
Nepal:
A study of group antenatal care in six villages in Achham found that among the control cohort, 8-10% of women could identify danger signs during pregnancy, labor and childbirth, or postpartum period.[28]
Nicaragua:
A study examining the impact of a radio-education intervention on knowledge of pregnancy danger signs found that the total number of signs identified by study participants increased by 53.8%, and found that urban setting and more than sixth-grade education were factors making it significantly more likely to score higher on post-test related to knowledge of danger signs.[29]
Nigeria:
A community-based survey in Osogbo metropolis found that 70.8% of women were aware of danger signs in pregnancy, with vaginal bleeding the commonest danger sign mentioned.[30] A cross-sectional study at the postnatal ward at Federal Teaching Hospital in Ebonyi found that most of the women knew about birth preparedness (87.7%) and complication readiness (79.5%).[31] A cross-sectional study of recently delivered women at selected health facilities in Ikenne found that 34.6% of women had knowledge of 5+ danger signs of pregnancy.[32] A cross-sectional study of pregnant women attending the prenatal clinic at a tertiary hospital found that 81.5% were “well prepared” for birth and its complications, however, only 27.4% knew key danger signs during labor/delivery and 24.9% knew those in the first 2 days after delivery.[33] A study of women in Zaria found that 18.31%, 9.89%, and 9.24% knew at least four danger signs during pregnancy, labor and delivery, and postpartum period, respectively.[34] A study evaluating the Maternal and Child Health Integrated Program (MCHIP) in Kano and Zamfara states found that mothers’ knowledge of birth preparedness/complication readiness was 32.2% among those who received counseling compared with 11.2% among those who did not.[35]
Pakistan:
A study in three rural areas around Islamabad found that the majority of women (75%) were unaware of key obstetric danger signs and symptoms, with traditional practices and home remedies commonly used to manage complications in pregnancy before seeking medical care, which was only done when the condition became unmanageable at home.[36]
Rwanda:
A study in 2015 at University Teach Hospital of Kigali of all admitted pregnancy-related complications found that the majority of first delays resulted from mothers failing to recognize the problem (22.3%). Women with hypertensive disorders represented 9.1% who failed to recognized signs of severity, followed by women who experienced abortive outcomes (abortion or ectopic pregnancy).[37] A cross-sectional study among pregnant women who were referred to Ruhengeri hospital between July and November 2015, found that out of 350 women, 296 (84.6%), 271 (77.4%) and 288 (82.3%) could mention at least one key danger sign during pregnancy, labor and postpartum respectively, but only 23 (6.6%) could mention three or more key danger signs during all three periods.[38]
South Africa:
A study of 340 pregnant women in KwaZulu-Natal found that although most of the study population (92%) attended health care facilities, only half (52%) of them knew about some of the “danger signs” of pregnancy, and 39% of them knew about their HIV status.[39]
Tanzania:
A community-based cross-sectional study of women who delivered in the previous two years in Chamwino found that 58.2% of respondents were considered to be prepared for birth and its complications, with maternal education a significant determinant of preparedness.[40] However, 68.6% of women knew 0 danger signs, with 6.1% knowing 1-4 and 25.2$ knowing 5+.[40] A follow-up study in Chamwino District found that 25.2% of respondents could mention at least five danger signs in any of the three phases of childbirth (pregnancy, childbirth, postpartum) with at least one in each phase, while 68.7% did not mention any danger signs.[41] A study of women who became pregnant or gave birth in the two preceding years in Mpwapwa found that 14.8% of women knew three or more obstetric danger signs, with the most commonly known signs including vaginal bleeding during pregnancy (19%), foul smelling vaginal discharge (15%), and baby stops moving (14.3%).[42] A study to evaluate the effectiveness of Home Based Life Saving Skills education found that the proportion of women who knew three or more danger signs improved substantially: 15.2% vs 48.1% during pregnancy, 15.3% vs 43.1% during childbirth, and 8.8% vs 19.8% in the postpartum period.[43] A study of women how had been pregnant in the past two years found that 51.1% knew at least one obstetric danger sign, with 26% knowing at least one danger sign during pregnancy, 23% during delivery, and 40% after delivery. However, few women knew three or more danger signs. Having secondary education was found to increase the likelihood of awareness of obstetric danger signs six-fold (OR=5.8, 95% CI 1.8-19.0) in comparison with no education at all.[44] A study of randomly selected pregnant women attending antenatal care in Dodoma municipality found that only 46.0% of women in the intervention and 44.7% of participants had knowledge on obstetric and newborn danger signs, rising to 77.3% after the intervention, compared to 48.0% in the control group.[45] A study in Kinondoni Municipality, Dar es Salam found that 57.8% of women were able to spontaneously mention only one to three danger signs, 31% had correct knowledge of at least four signs, and 2.7% were not able to mention any item.[46] However, among women who reported actually experiencing danger signs during their pregnancy (17.4% of respondents), 91% visited a healthcare facility.[46] The most commonly known pregnancy signs were vaginal bleeding (81%), swelling of the fingers, face, and legs (46%), and severe headache (44%), and older women were more likely to have knowledge of danger signs than young women (OR 1.61, 95% CI 1.05-2.46).[46]
Turkey:
A study of 125 pregnant women who had been admitted to the emergency department for antenatal bleeding found that advanced age, high level of education, lack of health insurance, receiving antenatal care, nuclear family structure, and knowledge of the danger signs during pregnancy were found to affect the use of emergency obstetric care services.[47]
Uganda:
A study of 810 women admitted in the antepartum period to Mulago hospital, found that only about 1 in 3 women were able to mention at least three of the five basic components of birth preparedness/complication readiness, and 1 in every 4 women could not mention any of the five components.[48] A study of 764 recently delivered women from 112 villages in Mbarara district found that 52% of women knew at least one key danger sign during pregnancy, 72% during delivery, and 72% during postpartum. Only 19% had knowledge of 3 or more key danger signs during the three periods. Overall 35% of the respondents were birth prepared. Young age and high levels of education had a synergistic effect on the relationship between knowledge and birth preparedness.[49] A study 0f 80 pregnant women attending antenatal clinic in Adjumani found that 76.25% of the respondents mentioned vaginal bleeding and 62.5% vomiting as danger signs in pregnancy, while 12.5% did not know any danger sign in pregnancy.[50]
Parameters
We used hierarchical logistic regression models to model the probability of recognition and referral. Based on findings in the literature, we assume that women with higher education are more likely to recognize and have the autonomy and necessary support to be referred. We also assume that more severe complications are more likely to be recognized and referred, and that recognition/referral probabilities increase with more advanced delivery site, with Home being the lowest, followed by Home-SBA, non-EmOC, BEmOC, and CEmOC. These constraints were enforced when sampling probabilities in the model. Based on the literature, we also assume that ANC visits improve the probability of recognizing complications for women delivering at Home (see ANC).
Priors
Model Implementation
If a delivery complication occurs, the probability of recognition/referral is drawn. A complication has to be recognized in order to be treated in the model, and depending on the woman’s current delivery site and the severity of the complication, she may be referred to another facility. Specifically, we assume that any complication that occurs at Home or non-EmOC will be referred, and any ‘severe’ complication that occurs at a BEmOC will be referred. Recognized complications that occur at a CEmOC facility are not referred. We currently assume that no false positives occur (i.e. 100% specificity).
References
- Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med 1994; 38(8): 1091-110. DOI: https://doi.org/10.1016/0277-9536(94)90226-7
- Geleto A, Chojenta C, Musa A, Loxton D. Barriers to access and utilization of emergency obstetric care at health facilities in sub-Saharan Africa: a systematic review of literature. Syst Rev 2018; 7(1): 183. DOI: https://doi.org/10.1186/s13643-018-0842-2
- Head SK, Yount KM, Sibley LM. Delays in recognition of and care-seeking response to prolonged labor in Bangladesh. Soc Sci Med 2011; 72(7): 1157-68. DOI: https://doi.org/10.1016/j.socscimed.2011.01.030
- Moran AC, Winch PJ, Sultana N, et al. Patterns of maternal care seeking behaviours in rural Bangladesh. Trop Med Int Health 2007; 12(7): 823-32. DOI: https://doi.org/10.1111/j.1365-3156.2007.01852.x
- Pervin J, Nu UT, Rahman AMQ, et al. Level and determinants of birth preparedness and complication readiness among pregnant women: A cross sectional study in a rural area in Bangladesh. PLoS One 2018; 13(12): e0209076. DOI: https://doi.org/10.1371/journal.pone.0209076
- Berhe AK, Muche AA, Fekadu GA, Kassa GM. Birth preparedness and complication readiness among pregnant women in Ethiopia: a systematic review and Meta-analysis. Reprod Health 2018; 15(1): 182. DOI: https://doi.org/10.1186/s12978-018-0624-2
- Geleto A, Chojenta C, Musa A, Loxton D. WOMEN’s Knowledge of Obstetric Danger signs in Ethiopia (WOMEN’s KODE):a systematic review and meta-analysis. Syst Rev 2019; 8(1): 63. DOI: https://doi.org/10.1186/s13643-019-0979-7
- Saaka M, Aryee P, Kuganab-Lem R, Ali M, Masahudu AR. The effect of social behavior change communication package on maternal knowledge in obstetric danger signs among mothers in East Mamprusi District of Ghana. Global Health 2017; 13(1): 19. DOI: https://doi.org/10.1186/s12992-017-0243-7
- Assaf S. Counseling and Knowledge of Danger Signs of Pregnancy Complications in Haiti, Malawi, and Senegal. Matern Child Health J. 2018; 22(11): 1659-1667. DOI: https://doi.org/10.1007/s10995-018-2563-5
- Kamineni V, Murki AD, Kota VL. Birth preparedness and complication readiness in pregnant women attending urban tertiary care hospital. J Family Med Prim Care 2017; 6(2): 297-300. DOI: https://doi.org/10.4103/2249-4863.220006
- Gopalakrishnan S, Eashwar VMA, Muthulakshmi M. Health-seeking behaviour among antenatal and postnatal rural women in Kancheepuram District of Tamil Nadu: A cross-sectional Study. J Family Med Prim Care 2019; 8(3): 1035-1042. DOI: https://doi.org/10.4103/jfmpc.jfmpc_323_18
- Akshaya KM, Shivalli S. Birth preparedness and complication readiness among the women beneficiaries of selected rural primary health centers of Dakshina Kannada district, Karnataka, India. PLoS One 2017; 12(8): e0183739. DOI: https://doi.org/10.1371/journal.pone.0183739
- Sharma N, Kumar N, Singh S, Malik JS, Jangra A. Status and determinants of birth preparedness and complication readiness in a rural block of Haryana. J Family Med Prim Care 2019; 8(2): 482-486. DOI: https://doi.org/10.4103/jfmpc.jfmpc_372_18
- Kochukuttan S, Ravindran TS, Krishnan S. Evaluating Birth Preparedness and Pregnancy Complications Readiness Knowledge and Skills of Accredited Social Health Activists in India. Int J MCH AIDS 2013; 2(1): 121-8. DOI: https://doi.org/10.21106/ijma.17
- Chandhiok N, Singh S, Chaudhury N, Shrotri A. Knowledge and Skills of Ayurvedic and Homeopathic Practitioners to Provide Skilled Birth Attendance in India: An Observational Study. Indian J Community Med 2018; 43(3): 175-179. DOI: https://doi.org/10.4103/ijcm.ijcm_280_17
- India Coverage Evaluation Survey 2009-2010. Ministry of Health and Family Welfare (India), ORG Centre for Social Research (ORG CSR), United Nations Children’s Fund (UNICEF). Available: http://ghdx.healthdata.org/record/india-coverage-evaluation-survey-2009-2010.
- Montgomery AL, Ram U, Kumar R, Jha P, Million Death Study Collaborators. Maternal mortality in India: causes and healthcare service use based on a nationally representative survey. PLoS One 2014; 9(1): e83331. DOI: https://doi.org/10.1371/journal.pone.0083331
- Raj SS, Maine D, Sahoo PK, Manthri S, Chauhan K. Meeting the community halfway to reduce maternal deaths? Evidence from a community-based maternal death review in Uttar Pradesh, India. Glob Health Sci Pract 2013; 1(1): 84-96. DOI: https://doi.org/10.9745/ghsp-d-12-00049
- Rosales A, Sulistyo S, Miko O, et al. Recognition of and care-seeking for maternal and newborn complications in Jayawijaya district, Papua province, Indonesia: a qualitative study. J Health Popul Nutr 2017; 36(Suppl1): 44. DOI: https://doi.org/10.1186/s41043-017-0122-0
- Mutiso SM, Qureshi Z, Kinuthia J. Birth preparedness among antenatal clients. East Afr Med J 2008; 85(6): 275-83. DOI: https://doi.org/10.4314/eamj.v85i6.9625
- Echoka E, Makokha A, Dubourg D, Kombe Y, Nyandieka L, Byskov J. Barriers to emergency obstetric care services: accounts of survivors of life threatening obstetric complications in Malindi District, Kenya. Pan Afr Med J 2014; 17 Suppl 1(Suppl 1): 4. DOI: https://doi.org/10.11694/pamj.supp.2014.17.1.3042
- Heerboth SA, Hennessey C, Omondi B, et al. Knowledge of Obstetric and Neonatal Danger Signs among Community Health Workers in the Rongo Sub-County of Migori County, Kenya: Results of a Community-based Cross-Sectional Survey. Afr J Reprod Health 2020; 24(1): 121-132. DOI: https://doi.org/10.29063/ajrh2020/v24i1.13
- Salem A, Lacour O, Scaringella S, et al. Cross-sectional survey of knowledge of obstetric danger signs among women in rural Madagascar. BMC Pregnancy Childbirth 2018; 18(1): 46. DOI: https://doi.org/10.1186/s12884-018-1664-x
- Kumbani L, McInerney P. The knowledge of obstetric complications among primigravidae in a rural health centre in the district of Blantyre, Malawi. Curationis 2002; 25(3): 43-54. DOI: https://doi.org/10.4102/curationis.v25i3.786
- Kumbani LC, McInerney P. Primigravidae’s knowledge about obstetric complications in an urban health centre in Malawi. Curationis 2006; 29(3): 41-9. DOI: https://doi.org/10.4102/curationis.v29i3.1092
- Ouasmani F, Engeltjes B, Raho BH, Belayachi O, Verhoeven C. Knowledge of hypertensive disorders in pregnancy of Moroccan women in Morocco and in the Netherlands: a qualitative interview study. BMC Pregnancy Childbirth 2018; 18(1): 344. DOI: https://doi.org/10.1186/s12884-018-1980-1
- Than KK, Morgan A, Pham MD, Beeson JG, Luchters S. Determinants of knowledge of critical danger signs, safe childbirth and immediate newborn care practices among auxiliary midwives: a cross sectional survey in Myanmar. BMJ Open 2017; 7(6): e017180. DOI: https://doi.org/10.1136/bmjopen-2017-017180
- Thapa P, Bangura AH, Nirola I, et al. The power of peers: an effectiveness evaluation of a cluster-controlled trial of group antenatal care in rural Nepal. Reprod Health 2019; 16(1): 150. DOI: https://doi.org/10.1186/s12978-019-0820-8
- Radoff KA, Levi AJ, Thompson LM. A radio-education intervention to improve maternal knowledge of obstetric danger signs. Rev Panam Salud Publica 2013; 34(4): 213-9. PMID: https://pubmed.ncbi.nlm.nih.gov/24301731/
- Sabageh AO, Adeoye OA, Adeomi AA, Sabageh D, Adejimi AA. Birth preparedness and complication readiness among pregnant women in Osogbo Metropolis, Southwest Nigeria. Pan Afr Med J 2017; 27: 74. DOI: https://doi.org/10.11604/pamj.2017.27.74.7266
- Onoh RC, Egede JO, Lawani LO, Ekwedigwe KC, Aja LO, Anozie BO. Birth preparedness and complication readiness among women of reproductive age group in Abakaliki, Southeast Nigeria. Niger J Clin Pract 2020; 23(3): 362-370. DOI: https://doi.org/10.4103/njcp.njcp_670_18
- Imaralu JO, Ani IF, Olaleye AO, Jaiyesimi E, Afolabi-Imaralu A, Odugbemi OO. Maternal and perinatal outcomes of birth preparedness and complication readiness in recently delivered women of a Southwestern Nigerian Town. Ann Afr Med 2020; 19(1): 60-67. DOI: https://doi.org/10.4103/aam.aam_29_19
- Aduloju OP, Akintayo AA, Aduloju T, Akin-Akintayo OO. Birth preparedness and complication readiness among prenatal attendees in a teaching hospital in South West Nigeria. Int J Gynaecol Obstet 2017; 139(2): 202-210. DOI: https://doi.org/10.1002/ijgo.12271
- George SO, Yisa IO, Alawode G. Knowledge of obstetric danger signs amongst women of reproductive age in PATHS2 Zaria cluster, Kaduna Nigeria. Niger J Med 2014; 23(1): 26-32. PMID: https://pubmed.ncbi.nlm.nih.gov/24946451/
- Ishola G, Fayehun F, Isiugo-Abanihe, et al. Effect of Volunteer Household Counseling in Improving Knowledge of Birth Preparedness and Complication Readiness of Pregnant Women in Northwest Nigeria. Afr J Reprod Health 2017; 21(1): 39-48. DOI: https://doi.org/10.29063/ajrh2017/v21i1.3
- Salam FT, Sarfraz M. Perceptions and practices among married women of child bearing age regarding obstetric danger signs in rural Islamabad: A qualitative study. J Pak Med Assoc 2018; 68(10): 1496-1501. Available at: https://jpma.org.pk/article-details/8892?article_id=8892
- Benimana C, Small M, Rulisa S. Preventability of maternal near miss and mortality in Rwanda: A case series from the University Teaching Hospital of Kigali (CHUK). PloS One 2018; 13(6): e0195711. DOI: https://doi.org/10.1371/journal.pone.0195711
- Smeele P, Kalisa R, van Elteren M, van Roosmalen J, van den Akker T. Birth preparedness and complication readiness among pregnant women admitted in a rural hospital in Rwanda. BMC Pregnancy Childbirth 2018; 18(1): 190. DOI: https://doi.org/10.1186/s12884-018-1818-x
- Hoque M, Hoque ME. Knowledge of danger signs for major obstetric complications among pregnant KwaZulu-Natal women: implications for health education. Asia Pac J Public Health 2011; 23(6): 946-56. DOI: https://doi.org/10.1177/1010539511428698
- Bintabara D, Mohamed MA, Mghamba J, Wasswa P, Mpembeni RNM. Birth preparedness and complication readiness among recently delivered women in chamwino district, central Tanzania: a cross sectional study. Reprod Health 2015; 12: 44. DOI: https://doi.org/10.1186/s12978-015-0041-8
- Bintabara D, Mpembeni RNM, Mohamed AA. Knowledge of obstetric danger signs among recently-delivered women in Chamwino district, Tanzania: a cross-sectional study. BMC Pregnancy Childbirth 2017; 17(1): 276. DOI: https://doi.org/10.1186/s12884-017-1469-3
- Urassa DP, Pembe AB, Mganga F. Birth preparedness and complication readiness among women in Mpwapwa district, Tanzania. Tanzan J Health Res 2012; 14(1): 42-7. DOI: https://doi.org/10.4314/thrb.v14i1.8
- August F, Pembe AB, Mpembeni R, Axemo P, Darj E. Effectiveness of the Home Based Life Saving Skills training by community health workers on knowledge of danger signs, birth preparedness, complication readiness and facility delivery, among women in Rural Tanzania. BMC Pregnancy Childbirth 2016; 16(1): 129. DOI: https://doi.org/10.1186/s12884-016-0916-x
- Pembe AB, Urassa DP, Carlstedt A, Lindmark G, Nyström L, Darj E. Rural Tanzanian women’s awareness of danger signs of obstetric complications. BMC Pregnancy Childbirth 2009; 9: 12. DOI: https://doi.org/10.1186/1471-2393-9-12
- Masoi TJ, Kibusi SM. Improving pregnant women’s knowledge on danger signs and birth preparedness practices using an interactive mobile messaging alert system in Dodoma region, Tanzania: a controlled quasi experimental study. Reprod Health 2019; 16(1): 177. DOI: https://doi.org/10.1186/s12978-019-0838-y
- Mwilike B, Nalwadda G, Kagawa M, Malima K, Mselle L, Horiuchi S. Knowledge of danger signs during pregnancy and subsequent healthcare seeking actions among women in Urban Tanzania: a cross-sectional study. BMC Pregnancy Childbirth 2018; 18(1): 4. DOI: https://doi.org/10.1186/s12884-017-1628-6
- Koşum Z, Yurdakul M. Factors affecting the use of emergency obstetric care among pregnant women with antenatal bleeding. Midwifery 2013; 29(5): 440-6. DOI: https://doi.org/10.1016/j.midw.2012.02.008
- Mbalinda SN, Nakimuli A, Kakaire O, Osinde MO, Kakande N, Kaye DK. Does knowledge of danger signs of pregnancy predict birth preparedness? A critique of the evidence from women admitted with pregnancy complications. Health Res Policy Syst 2014; 12: 60. DOI: https://doi.org/10.1186/1478-4505-12-60
- Kabakyenga JK, Östergren PO, Turyakira E, Pettersson KO. Knowledge of obstetric danger signs and birth preparedness practices among women in rural Uganda. Reprod Health 2011; 8: 33. DOI: https://doi.org/10.1186/1742-4755-8-33
- Florence M, Atuhaire C, Nkfusai CN, Shirinde J, Cumber SN. Knowledge and practice of birth preparedness and complication readiness among pregnant women attending antenatal clinic in Openzinzi Hciii, Adjumani District, Uganda. Pan Afr Med J 2019; 34: 46. DOI: https://doi.org/10.11604/pamj.2019.34.46.16869

GMatH (Global Maternal Health) Model - Last updated: 28 November 2022
© Copyright 2020-2022 Zachary J. Ward
zward@hsph.harvard.edu